Total Doses Distributed = 871,852,135. Total Doses Administered = 627,854,963. Number of People Receiving 1 or More Doses = 265,111,489. Number of People Fully Vaccinated = 226,200,755.
The Biden administration said Thursday that the COVID-19 public health emergency will continue through Jan. 11 as officials brace for a spike in cases this winter.
The decision comes as the pandemic has faded from the forefront of many people’s minds. Daily deaths and infections are dropping and people — many of them maskless — are returning to schools, work and grocery stores as normal.
The public health emergency, first declared in January 2020 and renewed every 90 days since, has dramatically changed how health services are delivered.
The declaration enabled the emergency authorization of COVID vaccines, testing and treatments for free. It expanded Medicaid coverage to millions of people, many of whom who will risk losing that coverage once the emergency ends. It temporarily opened up telehealth access for Medicare recipients, enabling doctors to collect the same rates for those visits and encouraging health networks to adopt telehealth technology.
Since the beginning of this year, Republicans have pressed the administration to end the public health emergency. President Joe Biden, meanwhile, has urged Congress to provide billions more in aid to pay for COVID-19 vaccines and testing. The federal government ceased sending free COVID-19 tests in the mail last month, saying it had run out of money.
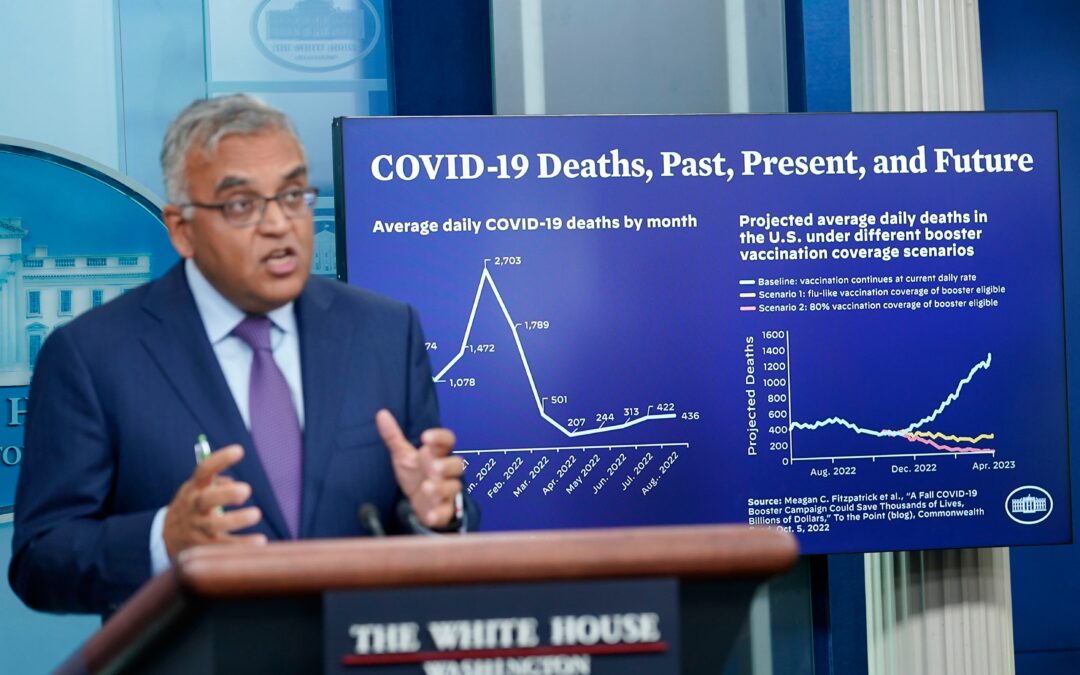
Public health officials are urging people age 5 and older to get an updated COVID-19 booster alongside a flu vaccine this fall before a predicted winter coronavirus surge and a nasty flu season. As of last weekend, about 13 million people had gotten the updated booster, which targets the omicron variant, according to White House COVID-19 coordinator Dr. Ashish Jha.
The administration has said it would provide 60 days notice before it ends the public health emergency.
___
Follow AP’s coverage of the pandemic at https://apnews.com/hub/coronavirus-pandemic
Indonesia’s leader launched the country’s first home-grown COVID-19 shot Thursday to help reduce the world’s fourth most populous nation’s dependency on imported vaccines.
President Joko Widodo announced the vaccine brand, IndoVac, as a new milestone of Indonesia’s pharmaceutical industry that will manufacture primary series vaccines, booster vaccines and vaccines for children, which have been in development since November 2021.
“From now on, we can produce our own COVID-19 vaccine,” Widodo said in an unveiling ceremony in West Java’s Bandung city. “And so we have independence in vaccine matters.”
During the ceremony, 15 residents who had not received any COVID-19 vaccine got their first IndoVac jabs.
Indonesia’s Food and Drug Authority greenlighted emergency use authorization of IndoVac in September, with an efficacy above 80% after two shots. The vaccine passed an audit by the country’s highest Islamic body that the shot is fit for consumption by Muslims — a particularly important factor in the world’s most populous Muslim nation.
IndoVac, made by inserting the genetic code for the antigen into yeast cells, is developed by state-owned pharmaceutical company Bio Farma in collaboration with U.S.-based Baylor College of Medicine, a private, independent health sciences center in Houston, Texas.
Widodo said Bio Farma plans to produce 20 million doses of primary series vaccine this year and 40 million doses next year as the company expands its facilities. In 2024, production may further increase to 120 million doses per year, depending on demand and the market.
As of Thursday, 73% of Indonesia’s 234.6 million people eligible for shots were fully two-dose vaccinated, and about 27% had a first booster dose while just 0.3% had a second booster.
Indonesia had largely recovered from its delta surge, which was among the worst in Southeast Asia. Last July, a then-record of about 56,700 daily new cases saw the delta variant overwhelming hospitals on the main island of Java. In February, omicron set a new high of over 63,900 new infections.
Though cases dropped steeply at the end of March and into April, they have recently been rising again with around 1,800 cases a day in the past week.
Overall, Indonesia has reported more than 6.4 million infections and 158,263 deaths from COVID-19. The actual numbers are widely believed to be higher.
Taiwan lifted all its COVID-19 entry restrictions on Thursday, allowing tourists unfettered access the self-ruled island after over 2 1/2 years of border controls.
Hong Kong and Taiwan, together with mainland China, long required most visitors to complete a mandatory quarantine period throughout the pandemic, even as most countries reopened their borders to tourists.
Visitors are no longer required to quarantine upon entry, or take any PCR tests. Instead, they will need to monitor their health for a week after arriving, and obtain a negative result on a rapid antigen test the day they arrive. If people want to go out during the weeklong monitoring period, they need a negative test from either that day or the day before.
There are also no longer any restrictions on certain nationalities being allowed to enter Taiwan.
Dozens of visitors from Thailand were among the first to arrive under the new rules at Taiwan’s Taoyuan International Airport, which serves the capital Taipei, on a Tiger Air flight that landed shortly after midnight.
Tourists like 32-year-old Mac Chientachakul and his parents were excited to visit the island.
“Hot pot is my favorite dish in Taiwan,” Chientachakul said. “It’s my first thing to do … I miss it so much.”
Sonia Chang, a travel agent, said the changes are good for both the the tourism industry and Taiwanese residents, who can now travel abroad without having to quarantine when they get home.
Valaisurang Bhaedhayajibh, a 53-year-old business development director of a design firm, called the new rules convenient.
“We don’t have to do the test before coming here, and also after arriving,” he said. “We are still required to do the self-test every two days, and everything has been provided” by Taiwanese authorities, including the rapid testing kits.
At a welcome ceremony in the Taoyuan airport’s arrival hall, the travelers from Thailand were met by the Taiwan Tourism Bureau’s director, Chang Shi-chung, who handed out gifts.
Taiwan’s tourism bureau estimated that a total of 244 tourists from some 20 tour groups will arrive Thursday.
With both Hong Kong and Taiwan getting rid of restrictions and welcoming back tourists, mainland China remains one of the few places in the world adamant in keeping borders closed and sticking to a “zero-COVID” strategy to stamp out the virus. Hong Kong ended its mandatory quarantine policy for inbound travelers late last month, requiring just a three-day self-monitoring period.
Now the Food and Drug Administration has given a green light for elementary school-age kids to get the updated booster doses, too — one made by Pfizer for 5- to 11-year-olds, and a version from rival Moderna for those as young as 6.
There’s one more step before parents can bring their kids in for the new shot: The Centers for Disease Control and Prevention, which recommends how vaccines are used, must sign off.
Americans may be tired of repeated calls to get boosted against COVID-19 but experts say the updated shots have an advantage: They contain half the recipe that targeted the original coronavirus strain and half protection against the dominant BA.4 and BA.5 omicron versions.
These combination or “bivalent” boosters are designed to broaden immune defenses so that people are better protected against serious illness whether they encounter an omicron relative in the coming months — or a different mutant that’s more like the original virus.
“We want to have the best of both worlds,” Pfizer’s Dr. Bill Gruber, a pediatrician, told The Associated Press. He hopes the updated shots will “re-energize interest in protecting children for the winter.”
The updated boosters are “extremely important” for keeping kids healthy and in school, said Dr. Jason Newland, a pediatric infectious disease specialist at Washington University in St. Louis.
Parents should know “there is no concern from the safety perspective with the bivalent vaccines, whether Moderna or Pfizer,” Newland added.
Only people who’ve gotten their initial vaccinations — with any of the original-formula versions — qualify for an updated booster. That means about three-fourths of Americans 12 and older are eligible. As of last weekend, only at least 13 million had gotten an updated booster, White House COVID-19 coordinator Dr. Ashish Jha estimated Tuesday.
To pediatricians’ chagrin, getting children their first vaccinations has been tougher. Less than a third of 5- to 11-year-olds have had their two primary doses and thus would qualify for the new booster.
This age group will get kid-size doses of the updated booster — and they can receive it at least two months after their last dose, whether that was a primary vaccination or an earlier booster, the FDA said.
Pfizer said it could ship up to 6 million kid-sized doses within a week of authorization, in addition to ongoing adult-dose shipments.
Until now, Moderna’s updated booster was cleared only for adults. Wednesday’s FDA action authorized the booster for teens as well as children as young as age 6.
As for even younger tots, first vaccinations didn’t open for the under-5 age group until mid-June — and it will be several more months before regulators decide if they’ll also need a booster using the updated recipe.
Exactly how much protection does an updated COVID-19 booster shot offer? That’s hard to know. Pfizer and Moderna are starting studies in young children.
But the FDA cleared the COVID-19 booster tweaks without requiring human test results — just like it approves yearly changes to flu vaccines. That’s partly because both companies already had studied experimental shots tweaked to target prior COVID-19 variants, including an earlier omicron version, and found they safely revved up virus-fighting antibodies.
“It’s clearly a better vaccine, an important upgrade from what we had before,” Jha said earlier this week.
Jha urged adults to get their updated shot in October — like they get flu vaccinations — or at least well before holiday gatherings with high-risk family and friends. People who’ve recently had COVID-19 still need the booster but can wait about three months, he added.
___
The Associated Press Health and Science Department receives support from the Howard Hughes Medical Institute’s Department of Science Education. The AP is solely responsible for all content.
Africa must plan to respond effectively to disease outbreaks without international help, a top public health official said Wednesday, warning that the continent of 1.3 billion people is “on its own” during pandemics.
As assistance often never materializes, African nations must plug gaps in their response to outbreaks as such as Ebola in Uganda, said Ahmed Ogwell, acting head of the Africa Centers for Disease Control and Prevention.
“This is not the first outbreak of the Sudan strain of Ebola virus here in Africa and particularly here in Uganda,” he said. “We, unfortunately, at this time do not have rapid diagnostics for this particular strain. Neither do we have the vaccines for it.”
Ogwell spoke in the Ugandan capital, Kampala, where African public health officials and others are meeting to plan cross-border cooperation in responding to Ebola.
Uganda declared an outbreak of Ebola on Sept. 20.
Africa’s 54 countries have not received adequate international support in recent health crises, according to experts. Countries had difficulty getting COVID-19 vaccines.
Ogwell lamented the failure of the international community to help African countries improve their capacity to test for monkeypox and control its spread. He said no help has come to Africa, where more monkeypox deaths have been reported this year than anywhere in the world.
“Recently, during the pandemic, when we saw the number of monkeypox cases growing here in Africa, we issued a global alert but no help came to Africa,” he said. “In fact, today, as we see the tail end of the pandemic, there’s still no help coming to Africa for monkeypox. This means that we need to check the reality that is with us, and the reality for us is that when a public health crisis is big, like the pandemic, Africa is on its own.”
The epicenter of Uganda’s Ebola outbreak is a rural community in central Uganda where health workers were not quick to detect the contagious disease that manifests as a viral hemorrhagic fever.
Although Ebola began spreading in August, officials initially described a “strange illness” killing people. Ebola now has infected 54 people and killed at least 19, including four health workers. One of its victims is a man who sought treatment in a hospital in Kampala and died there.
Ebola can be difficult to detect at first because fever is also a symptom of malaria. Ebola is spread through contact with bodily fluids of an infected person or contaminated materials. Symptoms include fever, vomiting, diarrhea, muscle pain and at times internal and external bleeding.
There is no proven vaccine for the Sudan strain of Ebola. But plans are underway to test a possible vaccine in a small group of Ugandans who had contact with Ebola patients.
Because Ebola is “a priority disease” for Africa, “the absence of rapid diagnostics and the absence of a vaccine means we have a gap in how we prioritize our diseases and the tools we need to respond to them,” according to Ogwell.
“As Africa, we must now do things differently, appreciating that for the most time we will be on our own. Knowing that we are on our own, though, needs to motivate us so that we can do things on our own but not alone,” he said. “We must plan, prepare and respond effectively using our own resources, including our experts and institutions, and we must produce the health products we have identified as a priority for this continent.”